

Missed calls pile up before lunch. A scheduler is toggling between appointment templates, refill requests, and a voicemail queue that never really clears. The physicians see a full day on the calendar and assume the practice is productive, but the staff feels buried, patients wait too long for answers, and small errors keep showing up in the chart.
That's the problem behind how to improve staff productivity in a medical practice. For independent dermatology, gastroenterology, and internal medicine groups, productivity is not about pushing people to move faster. It's about diagnosing where time is being lost, fixing workflow gaps, and choosing technology that reduces administrative drag without creating new work. Done well, you get better patient access, less staff strain, and a practice that runs with more control.
Meta description: How to improve staff productivity in a medical practice with better KPIs, workflow fixes, EMR optimization, and AI support that reduces admin burden.
First Diagnose the Real Productivity Gaps in Your Practice
The front desk usually looks like the problem. Phones ringing, patients checking in, refill messages waiting, portal tasks stacking up. But in most practices, the productivity drain sits behind the visible chaos. Staff spend large parts of the day on work that doesn't show up cleanly on a schedule, such as pharmacy callbacks, prior auth follow-up, incomplete intake chasing, duplicate documentation, and explaining the same prep instructions over and over.

A practice can look fully staffed and still be losing hours every day to invisible work. That's one reason generic advice about “working smarter” usually falls flat in healthcare. Productivity guidance often omits methods to quantify invisible work like phone callbacks or billing notes, and a 2023 AMA survey found nearly 60% of physicians reported burnout, driven by workload and lack of control (Lyra Health summary of AMA findings). If administrative volume isn't rebalanced, asking staff to be more efficient just adds pressure.
Track the work that never makes the schedule
Start with a one-week reality check. Not a broad “how busy are we” discussion. A simple log of interruptions, call reasons, handoffs, and repeat work.
Useful categories include:
- Phone burden: inbound calls, abandoned calls, refill requests, referral status checks, prep questions, lab result follow-up
- Scheduling friction: reschedules, late cancellations, appointment type errors, missing insurance information, patients booked into the wrong visit length
- Documentation drag: duplicate entry between call notes and EMR, incomplete intake, chart corrections, manual routing
- Exception handling: prior auth follow-up, pharmacy clarification, insurer requirements, after-hours messages that become next-day cleanup
Many managers are surprised to learn that the issue usually isn't staff idleness, but rather skilled staff doing fragmented work all day, with constant context switching.
Practical rule: If a task happens often, follows predictable rules, and still consumes staff attention every day, it belongs on your productivity audit.
Look for bottlenecks, not just busy people
In a GI clinic, one common bottleneck is prep and scheduling coordination. In dermatology, it may be triaging visit types and handling cosmetic versus medical scheduling rules. In internal medicine, refill requests and result follow-up can dominate the day. Every specialty has its own version of hidden load.
A simple review matrix helps:
| Operational area | What to look for | What it usually means |
|---|---|---|
| Calls | Long queues, repeated callbacks, after-hours backlog | Access failure, not staffing laziness |
| Scheduling | Wrong visit types, template confusion, empty slots beside long waits | Rule design problem |
| Intake | Missing forms, repetitive follow-up, day-of delays | Pre-visit process is weak |
| Refills and results | High message churn, repeated routing, manual clarifications | Clinical support workflow is fragmented |
If you want a broader non-healthcare perspective on documenting team friction and meeting overload, effective productivity for mid-sized agencies offers a useful lens. The setting is different, but the core idea holds up: teams lose output when no one measures where time goes.
Define What Productivity Means for Your Practice with KPIs
Once you know where the work is leaking, the next step is defining productivity in terms that matter to a practice. Speed alone is a bad metric. A short call that leads to a wrong appointment type or an incomplete refill is not productive. It just moves the problem downstream.
The better approach is to tie staff effort to patient access, task completion quality, and operational stability. That's where KPIs help. When organizations define SMART goals linked to KPIs, such as average call handling time, completed pre-visit intakes, or schedule fill rate, they see 15 to 25% improvements in targeted metrics over 6 to 12 months, especially when those goals are paired with structured feedback loops (StaffCircle).
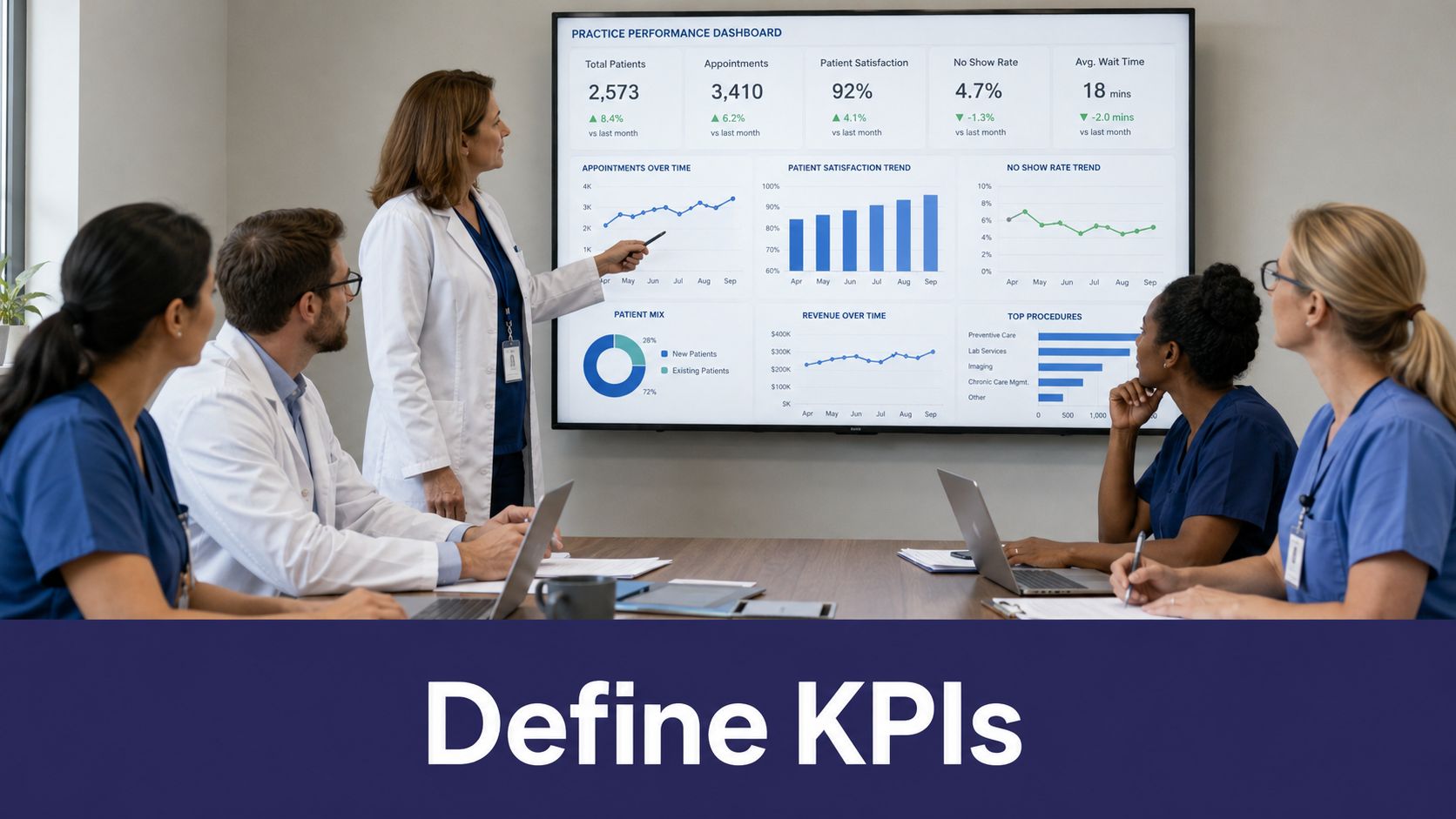
Choose KPIs that match the patient journey
Most small practices do better with a short list of tightly aligned metrics than a giant dashboard no one uses. For front-office and clinical support workflows, start with measures that answer one basic question: are we making it easier for patients to get what they need without creating more rework?
A practical KPI set might include:
- Call capture rate: are inbound calls getting answered and documented
- First-call resolution rate: how often does the patient get a complete answer without a callback
- Schedule fill rate: are templates being used well, including late cancellation recovery
- Completed pre-visit intake rate: are forms and history collected before the appointment
- No-show rate: is scheduling and reminder workflow improving attendance
- Refill turnaround consistency: are medication requests moving through a standard process
- Third-next-available appointment by visit type: are patients getting access
Avoid vanity metrics
A common mistake is choosing KPIs that are easy to count but don't reflect care operations. Raw call volume is one example. More calls handled can mean access is improving, or it can mean patients keep calling back because the first interaction failed.
The right KPI should help a manager decide what to fix next. If a metric can't guide action, it's probably noise.
Use a small scorecard for each role. Schedulers need different targets than refill coordinators. MA teams handling intake need different measures than front-desk staff handling check-in. Practices using eClinicalWorks, gGastro, EMA ModMed, Athenahealth, Epic, or DrChrono should build KPIs around what those systems can reliably record, not what sounds impressive in a meeting.
Review the numbers often enough to matter
Annual reviews won't improve daily operations. Weekly or fortnightly review works better because the team can still remember what caused the problem. A short rhythm is enough:
- Pick no more than a few priority KPIs per role.
- Compare current performance to the previous week.
- Note where the process broke, not just who struggled.
- Adjust scripts, templates, routing, or scheduling rules.
- Recheck the same metrics after the change.
That's how vague frustration turns into operational control.
Optimize Workflows and Reduce the Administrative Burden
Most productivity gains in medical practices come from redesigning work, not from asking the same team to absorb more. Once the bottlenecks are visible, map the current process exactly as it happens. Not how the policy manual says it works. The actual path.
That means tracing a refill request from patient call to EMR documentation to pharmacy action. It means following a new-patient scheduling call through insurance capture, appointment selection, intake completion, and chart prep. When practices use a structured process-improvement framework with current-state mapping and small tests, task cycle times can drop 25 to 40% and productivity gains of 20 to 30% are possible in service settings like healthcare (MIT Sloan).

Map the handoffs first
Most waste lives in the transitions. One person takes the message. Another checks the chart. A third calls the patient back. A fourth documents the outcome. By the end, four people touched one routine request.
A workflow map should answer:
- Where does the task start
- Who owns the next step
- What information is required to complete it
- Where does the process stall
- What forces manual re-entry or duplicate review
This exercise is especially useful for common high-volume processes:
- Appointment scheduling and rescheduling
- Pre-visit intake
- Prescription renewals
- Test result communication
- Post-op and chronic care follow-up
- Referral and order coordination
Remove repetitive work before adding more staff
The biggest administrative win usually comes from taking repetitive, rule-based work off the live phone line. That includes scheduling, patient intake, refill collection, basic education, reminder outreach, and status updates. A 2021 systematic review of 11 randomized controlled trials found automated, multi-modal appointment reminders reduced no-show rates by roughly 26% compared with no reminders, especially when sent at least 24 hours in advance (IBM summary).
That matters because every no-show, callback loop, and incomplete intake creates extra labor on top of the clinical schedule.
A busy front desk is often doing rework created by a weak workflow. Fix the workflow first, and staffing pressure changes quickly.
For practices evaluating automation, the useful question isn't “Can this answer the phone?” It's whether the tool can absorb a meaningful share of front-office and clinical support work inside your existing process. That includes inbound and outbound calls, intake, refill routing, chart documentation, pre-visit work, post-visit education, and chronic disease check-ins.
One option in this category is Simbie AI, which is positioned as AI Medical Staff rather than just an answering service. It covers both administrative and clinical support workflows, captures 100% of inbound calls, runs 24/7 with zero hold times, is HIPAA-compliant and SOC 2 Type 2 certified, and can reduce front-office staff costs by up to 60% while integrating into systems such as eClinicalWorks, gGastro, EMA ModMed, Athenahealth, Epic, and DrChrono. For a closer look at this workflow model, see healthcare workflow automation.
Test small changes before rolling them out broadly
Don't redesign everything in one month. Pick one workflow, one location, one call type, or one provider segment. Then measure what changed.
A good sequence is simple:
- Map the current workflow.
- Choose one friction point.
- Test one operational change.
- Review the result after a short interval.
- Keep, revise, or discard it.
That discipline prevents the classic mistake of making six changes at once and not knowing which one helped.
Implement Technology That Works With Your Practice Not Against It
Bad technology adds clicks, fragments responsibility, and makes staff do double entry. Good technology disappears into the workflow. That difference matters more than the feature list.
A lot of medical practices buy software based on a demo that looks efficient in isolation. The trouble starts after go-live, when staff realize the tool doesn't match appointment logic, can't write back into the chart cleanly, or creates another inbox to monitor. If you're serious about how to improve staff productivity, implementation should be judged by operational fit.
Integration matters more than novelty
A useful tool has to work with the systems your team already uses every day, including eClinicalWorks, gGastro, EMA ModMed, Athenahealth, Epic, and DrChrono. If scheduling, intake, or call documentation has to be copied manually from one screen to another, you haven't improved productivity. You've just moved the work.
Look for technology that can:
- Write directly into the EMR: intake details, call notes, refill requests, and task outcomes should land in the patient record without extra transcription
- Follow specialty-specific scheduling rules: dermatology, GI, and internal medicine all have different visit-type logic and duration needs
- Support both front-office and clinical tasks: not just answering calls, but helping with result communication, patient education, refill handling, and follow-up outreach
- Allow human takeover: staff should be able to monitor activity and step in when an exception needs judgment
Measure quality outcomes, not just activity volume
Many technology projects fail because the practice tracks what's easy instead of what matters. A McKinsey analysis found only about 20% of healthcare productivity projects track downstream metrics like appointment access or no-show rates, rather than relying on narrow KPIs alone (Performance Institute summary). That's exactly how teams end up celebrating faster call handling while patients still struggle to get scheduled correctly.
Use a before-and-after review that includes both operational and care-adjacent outcomes:
| What to measure | Weak approach | Better approach |
|---|---|---|
| Calls | Number answered | Resolved without manual follow-up |
| Scheduling | Appointments booked | Correct visit type and improved access |
| Intake | Forms sent | Intake completed before visit |
| Refills | Messages processed | Time to completed refill workflow |
| Follow-up | Outreach volume | Patient completion of next step |
Skeptical practice owners are usually right. Technology can make a dashboard look better while the day-to-day workload stays miserable. Don't accept volume claims without checking whether patient flow, chart quality, and staff burden improved.
Security is part of workflow design
In healthcare, security and productivity are tied together. If staff don't trust a tool, or if compliance review keeps stopping rollout, the technology will never become part of normal operations.
For that reason, basic requirements should be mandatory:
- HIPAA-compliant controls
- SOC 2 Type 2 certification
- Clear auditability
- Defined escalation paths for clinical or operational exceptions
Built-by-clinicians credibility also matters more than most vendors admit. Simbie AI was built by physicians from Stanford, Yale, Columbia, and Princeton, and that kind of background shows up in scheduling logic, documentation structure, and workflow judgment. The practical point is not prestige. It's whether the product understands how a medical practice runs. If you want to review what integration should look like in a real workflow, see EMR and system integrations for healthcare practices.
Empower Your Team Through Training Scheduling and Burnout Prevention
A practice does not become more productive just because software took over some tasks. The gain only becomes real when the team's role is redesigned around work that requires human judgment.
That means fewer staff hours spent trapped in repetitive phone loops, and more time spent on complex scheduling decisions, patient reassurance, care coordination, and exception handling. It also means looking at workload. If your team is “productive” only because everyone is absorbing constant interruption, the model won't hold.

Rebuild roles around higher-value work
Front-desk and administrative staff are often judged by how much they can juggle. That's the wrong standard. A better standard is whether they can complete the right tasks with consistency and less rework.
Once repetitive workflows are automated or standardized, retrain staff around responsibilities such as:
- Complex patient routing: cases where symptom context, insurance nuance, or visit urgency matters
- Care coordination: referrals, follow-up sequencing, and closing loops with outside facilities or pharmacies
- Patient communication: explaining prep steps, next actions, and non-urgent guidance clearly
- Quality checks: catching scheduling mismatches, incomplete charts, or exceptions before they disrupt clinic flow
Engagement is operational, not cosmetic
Staff engagement is often treated like an HR topic. In practice operations, it's a productivity issue. Employees who feel engaged are about 18% more productive than disengaged colleagues, and highly engaged workforces see an average 23% increase in profitability (ActivTrak).
The reason is straightforward. People do better work when expectations are clear, when they have tools that reduce friction, and when managers recognize what good performance looks like.
Recognition works best when it's tied to specific operational wins, such as cleaner intake completion, fewer scheduling errors, or stronger follow-through on refill workflows.
Scheduling should protect capacity, not just fill it
A packed day is not always a productive day. In many independent practices, overbooked templates and unpredictable phone volume force staff into continuous triage mode. That leads to mistakes, frustrated patients, and turnover risk.
A more stable model includes:
- Protected admin blocks: so refill, result, and callback work does not spill into every open minute
- Clear escalation lanes: staff should know which issues require physician review and which can be resolved through standing workflow
- Cross-training with limits: enough backup coverage to prevent bottlenecks, without making every role vague
- Capacity-aware staffing plans: based on hidden work, not just visible check-in volume
If your scheduling process itself is part of the strain, tools like healthcare staff scheduling software can help structure assignment, coverage, and workflow ownership more cleanly.
Measure Your Results and Create a Cycle of Continuous Improvement
The first round of changes is never the end of the job. Practices get into trouble when they launch new workflows, feel a short burst of relief, and then stop measuring. Three months later, old habits creep back in. Call queues rise again. Intake slips. Staff create manual workarounds. The system slowly returns to where it started.
Continuous improvement is what keeps productivity gains real.
Use a simple monthly review loop
Most practices don't need an elaborate operating system. They need a steady review habit. Pull your baseline metrics, compare them with current performance, and look for patterns in both output and workload quality.
A straightforward monthly review can include:
- Baseline check: compare current KPI performance with the pre-change period
- Workflow exception review: identify the tasks still requiring repeated manual rescue
- Staff feedback: ask where the new process still feels clumsy or incomplete
- Patient access view: review whether scheduling, no-shows, and callback burden are improving together
- One-change rule: commit to one operational adjustment before the next review
If you want a practical outside framework for building a review habit, Tooling Studio's team productivity guide is a useful reference for setting up measurable team performance without overcomplicating the process.
Watch for drift, not just failure
Most productivity problems return gradually. A scheduler starts bypassing the template because it feels faster. Intake gets documented later instead of before the visit. Refill requests begin piling up in a general inbox again.
That drift is why practices need process ownership. Someone has to review the workflow and ask whether the intended design is still being followed.
A short audit table can help:
| Review area | What to check monthly |
|---|---|
| Calls | capture, resolution, and repeat contacts |
| Scheduling | correct visit types, fill quality, late-cancel recovery |
| Intake | completion before visit, chart-readiness consistency |
| Clinical support | refill flow, result communication, follow-up completion |
| Team health | friction points, staffing strain, recurring bottlenecks |
Sustainable productivity is not a one-time cleanup. It's a management discipline.
Keep the system adaptable
Independent practices change quickly. A new payer requirement, a new provider, a different procedure mix, or an uptick in chronic care follow-up can break a workflow that worked well last quarter. That's why productivity systems should be flexible enough to adapt without forcing staff back into fully manual mode.
When that review cycle is built into the practice, improvement becomes normal work instead of a special project. For teams formalizing that discipline, healthcare process improvement resources can help structure the next round of workflow decisions.
If you're evaluating AI for your practice and want to see how clinically trained automation fits into real medical workflows, you can learn more from Simbie AI or see it in action at book a demo.