

The phone is still the most overloaded workstation in the pharmacy. It rings while a tech is counting, while a pharmacist is checking a DUR, while a patient is waiting at pickup, and while someone else wants to know if a refill is ready.
That pattern wears people down fast. It also creates the kind of constant task-switching that makes good staff feel like they can never finish one thing cleanly before the next interruption lands.
I’ve seen pharmacies try to solve this with more voicemail, longer hold queues, or a patchwork phone tree. Those fixes rarely hold. If you want a better answer, ai phone answering for pharmacy works best when you treat it as an operations project first and a tech project second.
The pharmacy phone that never stops ringing
Independent pharmacies are not dealing with a small nuisance. They are dealing with a daily volume problem. Independent pharmacies receive 100 to 300+ calls daily, and most of those calls are routine inquiries rather than work that needs a pharmacist’s direct attention, according to this pharmacy AI voice case discussion.
That aligns with what many teams already know from the bench. The calls are not usually unusual. They are repetitive.
A refill request. A “is it ready yet?” call. A question about store hours. A transfer. A basic insurance question. A reminder that a prior authorization is still pending. None of that is hard on its own. The problem is volume plus timing.
What the disruption looks like on the floor
The worst part is not just the ringing. It is the forced context switch.
A tech stops billing to answer a call about hours. A pharmacist pauses verification to answer a refill question that should have gone into a queue. Someone at the counter waits longer because the team is handling phone work in real time. Then the callback list grows because not every call gets handled fully on the first pass.
That is how a normal day turns into backlog.
Why old phone systems break down
Basic IVRs and voicemail boxes reduce some interruptions, but they usually create new work later. Staff still have to listen, sort, call back, document, and chase missing details. In practice, that means the phone burden gets delayed, not removed.
What works better is a system that can answer immediately, gather structured information, complete low-risk tasks, and pass along the rest with enough context to act. That is the difference between generic automation and healthcare-focused call handling.
Teams looking at broader medical call center workflows usually come to the same conclusion. The phone is not just a communication channel. It is an intake channel, a triage channel, and a task-generation channel. If you leave it unmanaged, it will run the day.
Tip: If your team says, “The phones are killing us,” start by auditing call reasons, not call duration. In pharmacies, the reason mix tells you far more than average handle time.
How an AI understands a prescription refill call
A good pharmacy voice agent is not a fancy voicemail box. It follows a structured process, and each step matters because errors at the start of the call carry forward.
Here is the basic flow.
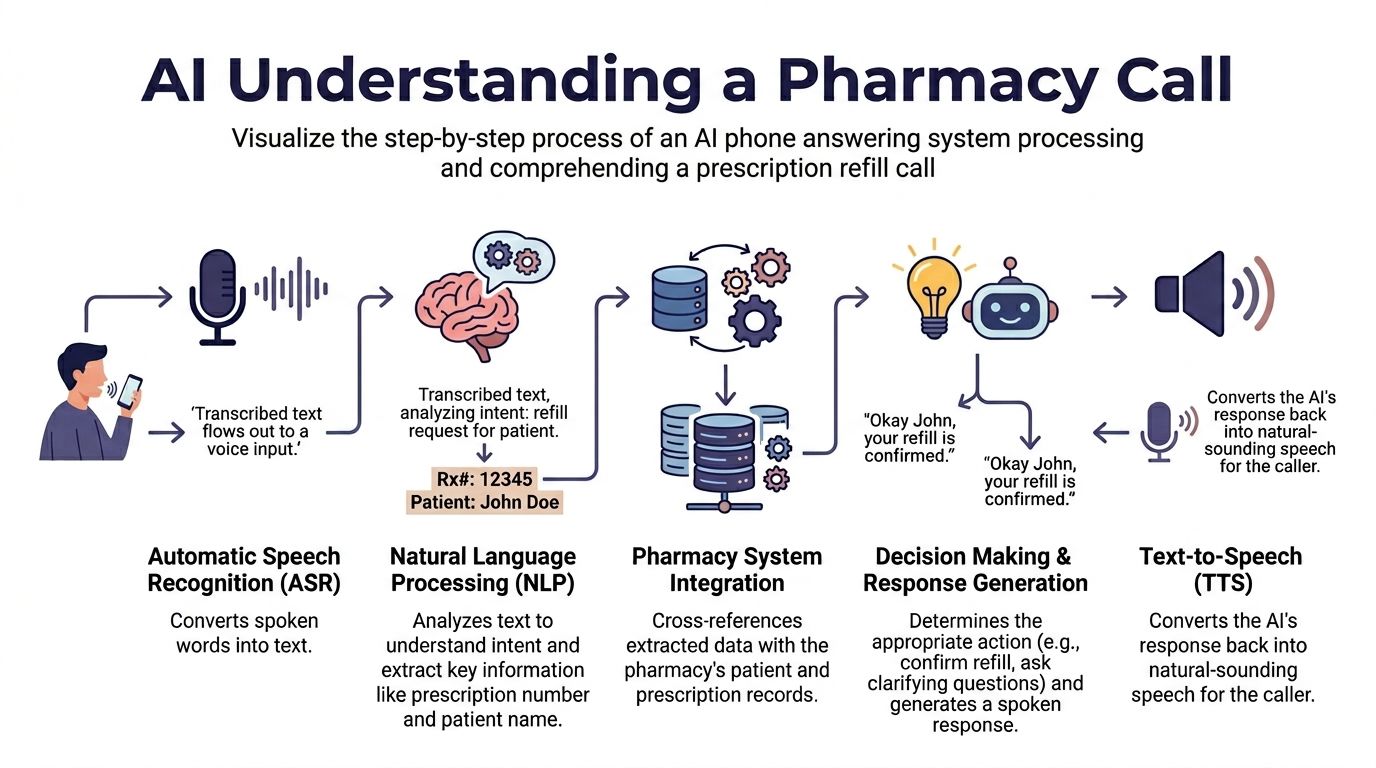
Step one is speech recognition
The first job is automatic speech recognition, or ASR. The system converts the caller’s speech into text.
That sounds simple until someone says “levothyroxine,” “amlodipine,” or “I need my blood pressure pills refilled, the little white ones.” Pharmacy calls are full of medication names, accents, background noise, and partial information, so generic speech tools often fall short.
Healthcare-trained models achieve low word-error rates in clinical settings, and that lower error rate comes from training on medical vocabulary. The same source notes that this significantly reduces transcription errors compared with generic models and makes reliable software integration possible. It also notes that 30% of inbound calls are routine refills, which is why accuracy at this first step matters so much for pharmacy automation, as explained in this overview of AI refills in healthcare and this analysis of ASR for prescription refill automation.
Step two is intent and data capture
Once the call is transcribed, the system determines what the caller wants.
Natural language processing is applied here. The agent identifies the intent, refill request, status check, store-hours question, transfer request, or something else, and pulls out the details attached to that request. Name, date of birth, prescription number, preferred pickup time, medication name, and callback number all get slotted into fields.
This is the part many people picture as “AI.” In reality, the best systems are not improvising. They follow a controlled workflow with prompts, validation steps, and business rules.
Step three is system lookup and decision logic
After the system knows the intent, it checks the pharmacy data it has access to. That might mean looking for a patient match, confirming whether a prescription is ready, or seeing whether the refill request should enter a queue for staff review.
A well-built voice flow does not guess when the data is thin. It asks follow-up questions. If the phone number suggests a likely patient match, the system can use that as a starting point, then validate identity with prompts such as date of birth before taking action.
Step four is response or handoff
At the end, the AI either responds directly using text-to-speech or hands the task to a human.
For a routine question, the agent can answer right away. For a refill request, it may create a structured task in the pharmacy workflow. For a clinical issue, it should stop and route the call out.
That is why I prefer systems with visible call logic, transcripts, and task outputs. The black-box approach sounds impressive in demos, but pharmacies need an auditable process.
Practical use cases beyond simple prescription refills
Pharmacies get the most value when they stop thinking about AI as “the refill bot” and start thinking about it as front-end phone operations. Refill capture is the obvious use case, but it is not the only one worth automating.

Routine calls are the first layer
The easiest wins come from taking routine traffic off the bench.
That includes:
- Refill intake: The system gathers patient identifiers, medication details, and preferred timing, then routes a complete request instead of a vague voicemail.
- Status checks: If the pharmacy system can provide status data, the caller can hear whether a prescription is in process, ready, or needs follow-up.
- Hours and store information: Calls about hours, location, holiday closures, and pickup basics should never interrupt clinical work.
- Basic insurance and transfer questions: The AI can capture enough detail to start the right task and avoid repeated back-and-forth.
Triage is where the workflow gets better
Here, strong systems pull ahead. AI voice agents can resolve simple inquiries on their own and forward complex ones to a human with full context. That model has shown 30% faster call completion and 10% higher quality scores than human-only agent models, according to Infinitus benchmarks on healthcare call triage.
That matters because the value is not just call containment. The value is cleaner routing.
A pharmacist should not answer ten basic status calls before getting to the one person reporting a side effect. A tech should not hunt through scraps of voicemail for the patient’s date of birth because the original intake was incomplete. Better triage fixes both problems.
For teams comparing options, I usually frame it like this.
| Workflow | Before | After |
|---|---|---|
| Refill requests | Staff answers live or calls back from voicemail | AI captures details and queues a refill task |
| Order status | Staff interrupts bench work to check status | AI answers directly if status data is available |
| New patient intake | Front desk gathers details manually | AI collects core information before staff follow-up |
| Clinical questions | Mixed in with routine traffic | AI routes these directly with context |
You can see similar patterns in voice AI healthcare operations, where the gain comes from sorting work by risk and complexity rather than treating every incoming call the same way.
Higher-value use cases that are often missed
Some pharmacies stop after inbound call handling. That is leaving value on the table.
I’ve seen better results when the phone system also supports:
- Prior authorization follow-up: The system can start outbound status checks or collect the right details before staff steps in.
- Refill reminders and adherence outreach: These outbound calls can reduce inbound traffic and pull patients back into a predictable refill cycle.
- Pickup notifications or basic follow-up calls: These work best when the message is structured and the escalation path is clear.
- Doctor-line prioritization: Some pharmacies give prescriber calls a different path so they do not sit behind routine patient traffic.
Key takeaway: The best pharmacy voice setup does not try to answer everything. It removes simple work, isolates risky work, and hands the team a cleaner queue.
Key benefits and how to calculate your ROI
A pharmacy usually feels the payoff from AI phone answering in labor recovery first. The bigger win is operational control. Calls get answered during rush periods, refill traffic stops breaking bench focus, and staff can stay on work that requires a licensed human or an in-person handoff.
The financial case is strongest when the pharmacy already has steady call volume and frequent interruptions. In that setting, the goal is usually to remove phone drag from existing staff, who are already juggling multiple roles, rather than replacing a dedicated receptionist.

Where the return comes from
I break ROI into four buckets.
- Staff time recovered: Fewer interruptions for refill status, store hours, pickup questions, and basic routing.
- Better coverage during peaks: Calls still get answered at lunch, after work, and during the late-day refill rush.
- Lower rework: Staff starts with captured information instead of replaying voicemail and calling back to collect basics.
- More productive pharmacist and technician time: Verification, counseling, vaccines, compounding, and problem-solving get less interruption.
Only the first bucket drops neatly into a spreadsheet. The others show up in cleaner workflows, shorter callback queues, and fewer abandoned calls.
A simple ROI model you can use
Start with a model that your pharmacy manager or owner can check in ten minutes. If the assumptions are too complicated, the model will not survive the first budget meeting.
Use this formula:
(Hours of staff time saved per day × average hourly wage × days open per year) + value of calls captured that would otherwise be missed – annual AI service cost = annual ROI
That formula is simple on purpose. It gives you a practical first pass before you get into call transcripts, queue design, and integration scope.
| Input | What to measure |
|---|---|
| Staff time saved | Sample one or two weeks of refill, status, hours, and transfer-related calls |
| Hourly wage | Use the blended loaded cost of the employees who currently handle phone work |
| Days open | Use your real operating calendar, including shorter weekend hours if applicable |
| Captured calls value | Estimate the refill requests, transfer opportunities, or new patient calls that currently fall through |
| AI service cost | Use the full annual contract value, including setup, integrations, and any usage fees |
A quick example helps. If a pharmacy saves 2 staff hours per day, pays a blended loaded rate of $24 per hour, and operates 300 days a year, that is $14,400 in recovered labor capacity before you count missed-call capture. If the system costs $9,000 per year, the labor case alone is positive. If the pharmacy’s real savings are only 45 minutes per day, the math changes fast. That is why baseline measurement matters.
Where ROI estimates usually break down
The first mistake is overstating containment. No AI phone system closes every call end to end. Some calls still need a technician callback, pharmacist review, or manual exception handling.
The second mistake is ignoring implementation friction. If the phone agent is not connected to real pharmacy data, it can create extra work by collecting information staff still has to verify or re-enter.
The third mistake is using vendor averages instead of your own call mix. A high-volume store with repetitive refill traffic will usually see faster returns than a specialty operation with more complex clinical questions.
A scale example, and what independents should take from it
Large chains have already shown that pharmacy call automation can work at serious volume. A major U.S. retail pharmacy chain with over 7,000 store locations deployed AI voice technology to manage more than 1 million pharmacy-related calls per day, shifting roughly 120 inbound calls per store per day to automated voice support. The deployment used English and Spanish support and caller recognition with validation prompts for identity checks, according to this enterprise pharmacy voice deployment case.
An independent pharmacy does not need chain-level infrastructure. It does need disciplined scope. Start with high-volume administrative calls, measure labor recovered after go-live, and audit how many calls still need human follow-up. That is how you get to a real ROI number instead of a demo-day estimate.
Navigating clinical and regulatory responsibilities
At 5:47 p.m., the queue is backing up, two pickup windows are full, and the phone takes a call from a patient who says a new antibiotic is causing a rash. That is the moment to judge a pharmacy AI phone system. Not by how natural the voice sounds, but by whether it captures the basics, flags the risk, and gets a pharmacist involved fast.
This part gets glossed over in too many demos. Pharmacy phone automation touches protected health information and sits close to medication workflows. A bad setup creates privacy exposure, bad handoffs, and patient safety risk.
HIPAA is a workflow requirement
If a vendor says “HIPAA-friendly,” keep asking.
Ask how audio, transcripts, and structured data are encrypted in transit and at rest. Ask who can access recordings, whether access is role-based, what the audit logs capture, how long transcripts are retained, and whether the vendor will sign a Business Associate Agreement. Ask where data goes when the system records, transcribes, summarizes, or writes back into your pharmacy platform.
I usually ask vendors to map the full path of patient data from the phone call to the final system of record. Good vendors can do that clearly. If the answer stays vague, the risk is already too high.
The pharmacist needs clear override authority
A safe system’s role is limited to intake, classification, lookup, scripting, and routing. It does not practice pharmacy.
That boundary matters because pharmacy calls split into two very different groups. Administrative requests, such as refill status, store hours, or pickup questions, can often be handled within a controlled script. Clinical questions cannot. Side effects, allergy concerns, interaction questions, dose confusion, missed doses, worsening symptoms, and post-discharge medication issues need licensed review.
For this reason, any pharmacy system needs explicit override paths, fast warm transfer options, and auditable handoff logs, as discussed in this analysis of pharmacy AI handoff risk.
What good escalation rules look like
The best escalation logic is simple enough for staff to explain without opening a training binder.
Escalate immediately for:
- Allergy or reaction concerns: Rash, hives, swelling, breathing trouble, or any statement that a medication may be causing harm.
- Drug interaction questions: Especially if the caller mentions multiple drugs, supplements, a recent hospital discharge, or a medication change.
- Dose confusion: Any sign the patient is unsure what to take, when to take it, or whether they took too much.
- Clinical deterioration: Symptoms getting worse, medication not helping, or concern after starting a new therapy.
- Unclear intent: If the system cannot classify the call with confidence, it should hand off early.
The handoff should give the pharmacist a usable starting point. That usually means the transcript, caller identity data that was captured, the intent label, the reason for escalation, and the recording if your policy allows it. Staff should not have to restart the intake from zero unless the transcript is unreliable.
Build the stop-and-escalate list before go-live. If the clinical boundary stays loose, the system will drift into calls it should never finish on its own.
Audit trails matter more than voice quality
A polished voice helps adoption. A clean audit trail protects the pharmacy.
Supervisors need to see what happened on a call, what the agent captured, what action it took, who accessed the record, whether the call was transferred, and where the workflow failed. That is how teams catch bad routing rules, retrain scripts, and investigate complaints. It is also how pharmacies show that the process was controlled instead of improvised.
My rule is simple. If a workflow cannot be audited, it should stay with staff.
Your implementation and integration checklist
A solid launch is less about flipping the phone line over and more about making sure the operational plumbing is right. Most bad deployments fail because the pharmacy skipped workflow design and moved straight to voice prompts.

Start with call mapping
Before you talk to vendors, review your recent calls and sort them by reason.
Look for the repeat categories that create the most interruption. Refill requests, status checks, store information, transfer requests, prescriber calls, clinical questions, and after-hours messages should each have their own path. If you skip this step, you will end up buying a system that sounds good but routes badly.
Build the workflow before the script
A pharmacy script is only as good as the task path behind it.
Use a checklist like this:
- Identify top call types: Pull a call sample and rank by volume and staff burden.
- Define red-flag escalations: List the clinical situations that always go to a pharmacist or on-call process.
- Set data requirements: Decide what must be captured for each workflow, such as DOB, Rx number, medication name, callback number, or pickup preference.
- Map task destinations: Every call outcome should land somewhere specific. Refill queue, technician queue, pharmacist callback, voicemail fallback, or prescriber line.
- Test with messy real-world scenarios: Use accents, background noise, partial medication names, and impatient callers. Pharmacies do not get clean demo calls.
Plan the integration work carefully
At this point, many “AI answering” products turn into message-taking tools. If the system cannot read from or write to the software your team uses, staff will still do manual re-entry later.
Ask these questions early:
| Integration question | Why it matters |
|---|---|
| Can it verify patient identity using available context? | Reduces duplicate records and bad routing |
| Can it pull basic prescription status? | Lets the AI answer more than generic FAQs |
| Can it create a refill task in the right queue? | Avoids manual transcription from voicemail |
| Can it tag clinical escalations clearly? | Helps pharmacists prioritize correctly |
Train staff on the new division of labor
Staff training is often skipped because the project gets framed as “the AI will answer calls.” That is not enough.
Your team needs to know what the AI handles, what it never handles, how to review escalations, where transcripts live, how to correct errors, and who owns post-launch changes. If nobody owns tuning, the phone agent will stay stuck at day-one quality.
I also recommend a phased rollout. Start with routine FAQs and refill intake, then add more complex routing once the pharmacy trusts the outputs.
How to choose the right AI phone answering vendor
Most vendor evaluations go wrong because the demo focuses on voice quality instead of pharmacy fit. A polished conversation is nice. The harder questions are about safety, integration, and control.
Use a pharmacy scorecard
I like to score vendors in five areas.
- Pharmacy workflow fit: Have they handled pharmacy use cases before, or are they adapting a generic healthcare script?
- Data and compliance posture: Will they sign a BAA, and can they explain their logging, retention, and access controls clearly?
- Integration depth: Can they connect to your pharmacy management system in a way that reduces manual work instead of adding it?
- Escalation safety: Do they have fixed rules for allergies, side effects, drug interactions, and other high-risk calls?
- Admin control: Can your team change prompts, hours, routing, and escalation rules without opening a support ticket every time?
Multi-language support needs real proof
This issue gets ignored too often. A vendor may say they support multiple languages, but that can mean anything from basic prompt translation to reliable clinical call handling.
A 2025 NACDS study reported that 40% of U.S. pharmacy patients speak non-English primary languages, and miscommunications cause 15 to 20% of refill errors. That is why I tell pharmacies to ask vendors for benchmarked intent-recognition accuracy in the languages they need, not just a “yes” on a feature checklist, as noted in this review of pharmacy AI and multi-language support.
Questions worth asking in the sales call
Use direct questions. Do not settle for polished generalities.
- Show me how you handle a refill call with an unclear medication name.
- Show me where an allergy question gets stopped and escalated.
- Show me the staff view of the transcript and task output.
- Show me what happens if the caller speaks Spanish or mixes English and Spanish.
- Show me how my team edits hours, closures, and routing rules.
A vendor that can answer those well is usually worth a serious second meeting. One that cannot usually turns into more cleanup work for your staff.
Frequently asked questions about AI in the pharmacy
Will patients hate talking to AI
Some will notice it. Most care more about getting help fast than about whether a human picked up first.
The bigger factor is design. If the voice agent gets to the point, handles routine needs cleanly, and transfers quickly when the call is complex, patients usually adapt. Long, scripted conversations with too many prompts are what make people angry.
Can AI handle after-hours calls safely
Yes, if the after-hours scope is narrow and the escalation rules are strict.
Routine refill capture, hours, store information, pickup details, and callback intake are usually a good fit. Clinical advice, urgent symptom questions, and medication safety concerns should route to the human process you already trust.
How long does implementation take
That depends on workflow complexity and integration depth, so I would not promise a fixed timeline without seeing the pharmacy setup.
A simple launch with FAQ handling and refill intake is much easier than a build that includes status lookup, multilingual support, prescriber routing, and multiple locations. The more systems you connect, the more testing you need.
What is the best first use case
Start with the highest-volume, lowest-risk calls.
For most pharmacies, that means store information, refill intake, prescription status, and basic transfer capture. Once those are stable, add other workflows one by one.
What should I watch in the first month
Review transcripts, missed intents, escalation quality, and whether staff is receiving usable task data.
Do not judge success only by containment. Judge it by whether the pharmacy team spends less time chasing missing details and more time doing work that requires them.
If your pharmacy is trying to reduce phone burden without handing clinical judgment to a black box, Simbie AI is worth a look. It is built for healthcare voice workflows, with support for refill requests, intake, routing, and EMR-connected call handling. The best next step is to map your top call types, define your red-flag escalations, and then see how a healthcare-specific platform would fit your actual phone flow.